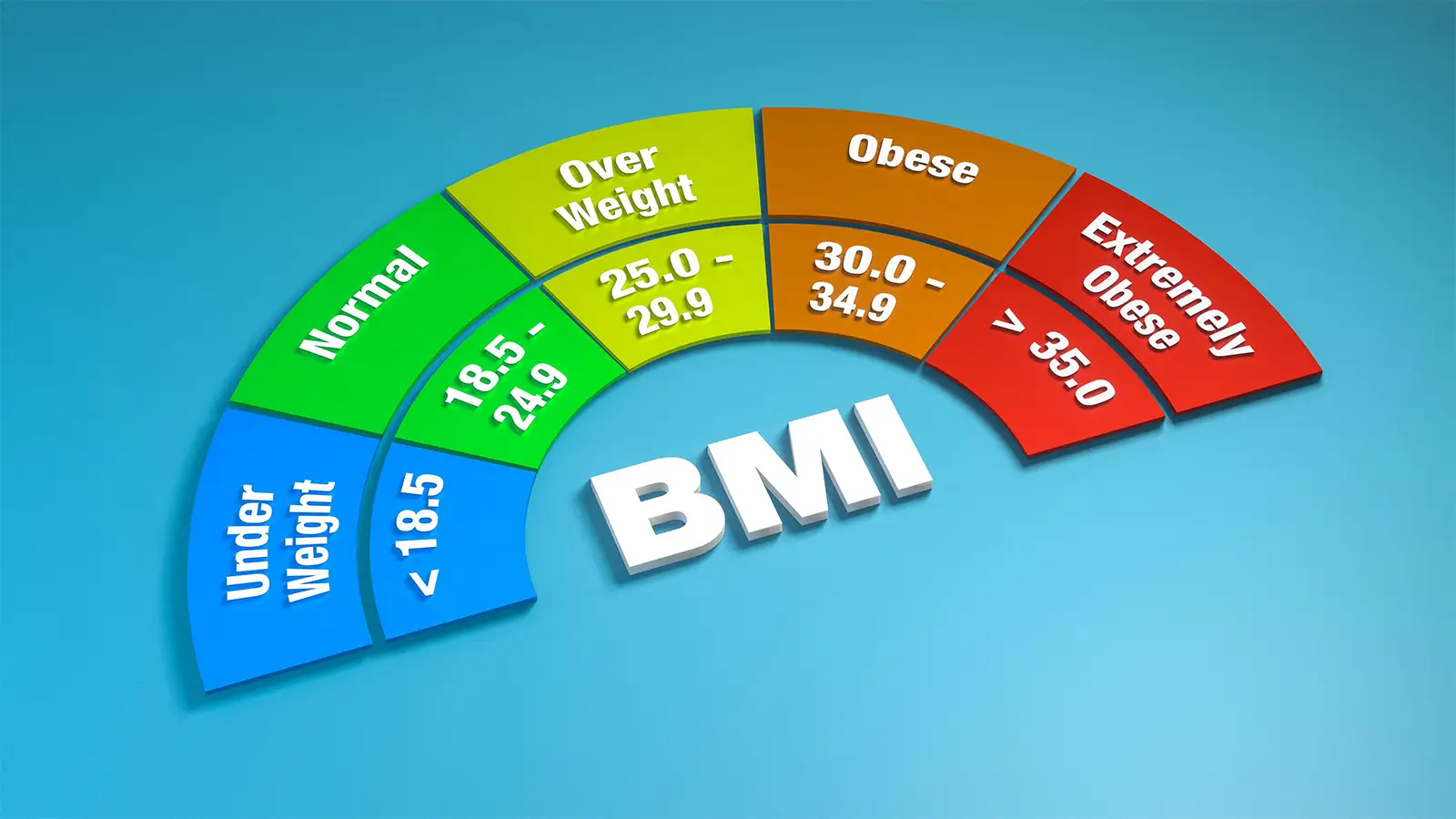
Moving away from body mass index (BMI) alone to diagnose obesity may delay treatment for millions of patients, a group of experts from the Endocrine Society warned in a guideline communication.
In January 2025, a Lancet Diabetes & Endocrinology global commission pitched a new framework that called for a more nuanced approach to diagnosing obesity. In theory, this would reduce misclassification and open the door for more personalized care.
Instead, the diagnostic overhaul may overcomplicate routine clinical care, argued Ranganath Muniyappa, MD, PhD, of the National Institute of Diabetes and Digestive and Kidney Diseases in Bethesda, Maryland, and colleagues in the Journal of Clinical Endocrinology & Metabolism.
“How obesity is defined has real consequences for patients. Diagnostic definitions influence who qualifies for treatment, how clinicians manage care and how insurers determine coverage for medications and surgery,” Muniyappa said in a press release. “Any new framework must be grounded in strong evidence, practical for everyday clinical use and designed to improve, rather than restrict equitable access to effective obesity treatment.”
Instead of relying solely on BMI, a tool that’s drawn much criticism over the years, the Lancet commission advocated that at least one other metric of body fat — like waist circumference, waist-to-hip ratio, waist-to-height ratio, or direct fat measurement — be included.
The commission also proposed splitting the diagnosis into two tiers: clinical obesity, defined by excess adiposity alongside organ dysfunction or functional limits, and preclinical obesity, where excess fat is present but clinical complications have not yet emerged.
Muniyappa’s team highlighted three main concerns with this framework:
- The practical difficulty of proving that organ dysfunction is directly caused by excess fat, which could stall timely weight-management interventions
- The conceptual challenges of defining preclinical obesity and the exclusion of type 2 diabetes from the list of obesity-induced organ dysfunctions
- The lack of standardization and accuracy among anthropometric measures of adiposity in most primary care settings
If the proposed framework were put into play, people with preclinical obesity who don’t have demonstrable functional impairment may be barred from early pharmacological invention, Muniyappa and colleagues said.
Currently, a BMI of 30 or higher is the standard for an obesity diagnosis; this group represents the largest pool of nondiabetic Medicare beneficiaries. If coverage were limited only to those meeting the “clinical obesity” definition, this population would shrink by approximately 20%, Muniyappa and co-authors pointed out.
The effect would be stark for the commercially insured population, too. Under current BMI standards, approximately 45% of commercially insured adults without diabetes — roughly 63 to 70 million people — qualify for obesity treatment. With the Lancet commission’s framework, that eligibility would be slashed by roughly half.
“It is reasonable to interpret part of the commission’s intent as prioritizing treatment for individuals with the greatest demonstrable health burden, particularly in the context of constrained payer resources. Targeting therapy toward those most likely to benefit is a defensible policy goal,” Muniyappa and colleagues said. “Our concern is less about prioritization itself and more about whether the proposed diagnostic structure is the optimal mechanism for achieving that goal, particularly given the central role of price and affordability in determining real-world access.”
Routine assessment of organ dysfunction or functional limitations also exceeds the capacity of most primary care settings, they noted. Because detailed diagnostic assessments are often unavailable in low-income, rural, and minority-serving settings, these stringent criteria risk worsening existing healthcare disparities.
“As a result, BMI combined with comorbidity status will remain the default classification tool because of its simplicity, scalability, and integration into electronic health records,” Muniyappa’s group wrote.
Instead of “rigid diagnostic thresholds,” they advocated for greater adoption of already established staging systems that incorporate clinical factors beyond BMI, such as the Edmonton Obesity Staging System (EOSS), the American Association of Clinical Endocrinology (AACE) Adiposity-Based Chronic Disease (ABCD), and the European Association for the Study of Obesity (EASO) models.
“Achieving harmonization across frameworks will require structured collaboration among professional societies, patient representatives, payers, and regulators,” Muniyappa and colleagues noted. “Pragmatic alignment may be more achievable than full definitional consensus and would reduce variability in clinical practice.”
Source: Read Full Article